1. What are the common chemicals which cause harm to the eye?
Common chemicals can be subdivided into alkali or acids.
Alkali burns are more dangerous due to high penetrating power into the eye. More the pH of alkali, the more harm it will cause to the eye. Common alkali agents are Lime, hydroxides of ammonia, Potassium hydroxide etc.
Acid burns, resulting from chemicals of low pH are usually less severe than alkali. Lesser severity is due to lesser penetration into the eye. Common acids are sulfuric acid, hydrochloric acid, nitric acid, acetic acid and hydrofluoric acid.
2. How much is the importance of “first aid” in chemical injuries to the eye?
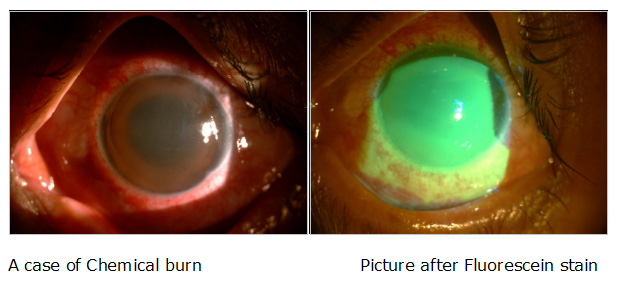
First aid is the most important step in the management of chemical injury to the eye. Even before rushing to eye specialist, anyone can give a thorough wash with normal tap water also. Ideally the patient should rush to the nearby eye specialist for first aid, where thorough saline wash must be given. Litmus paper can be used at the end of saline wash, to make sure that the pH is neutral.
A thorough examination of the involved structures is then carried out with a good illumination, preferably on slit lamp and the extent of damage is assessed. Any particles, especially in cases of lime are picked up with a forceps or a cotton bud. Deep impacted foreign bodies are removed in operation theatre under microscope.
3. What is autohemotherapy ?
In this technique, 0.5 to 1.5ml of the patient’s own venous blood is drawn from the vein and is injected under the conjunctiva in the perilimbal region and fornices. This is repeated every alternate day or as per requirement. The aim of this therapy is manifold. Blood acts as a barrier against deeper penetration of chemical. This is very useful in severe alkali burns. The fibrinolytic action of blood tends to inhibit the formation of symblepharon and it acts as a cushion in between the superficial and deeper tissues.
4. What is Amniotic Membrane Transplant in Chemical burn of eye?
Recent study suggests that amniotic membrane grafts in the early stages significantly reduced overall morbidity of chemical burns lesions. Amniotic membrane down regulates inflammatory processes and up regulates healing processes. It also provides an ideal substrate for epithelial cells to grow over it and populate the areas of epithelial defects.

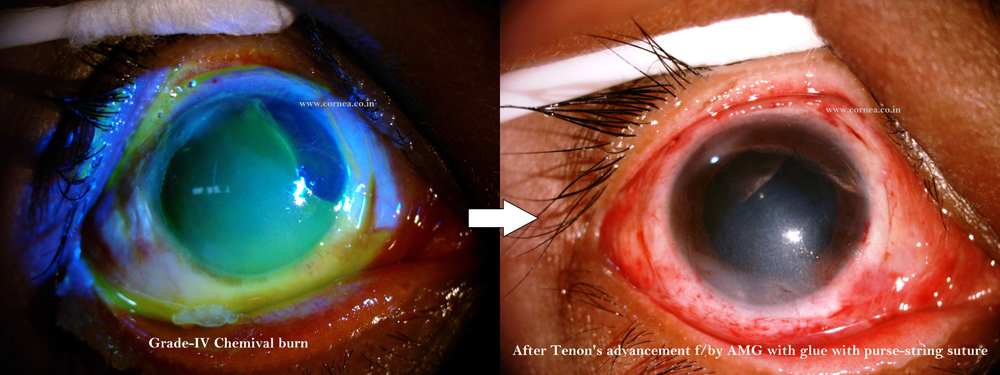
5. What is Tenoplasty ?
Tenoplasty or Tenon’s advancement is done in Moderate to severe grade of chemical injury of eye where some quadrant of eye is completely burnt (Seen as Blanching, as opposed to Redness). Here the purpose is to Bring Vascularisation to the blanched area. Tenoplasty could be potential eye saving procedure in cases of severe chemical inury.
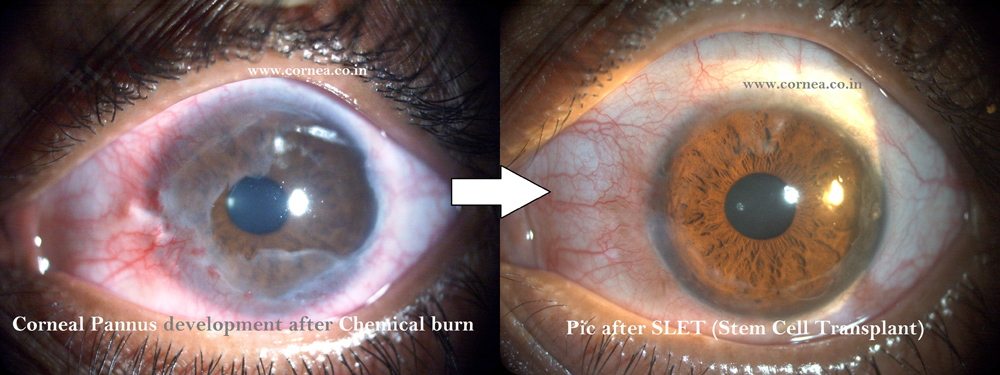
6. What is “stem cell transplant” surgery in chemical burn of eye?
It is now well established that stem cells for the cornea as well as conjunctival epithelium are located in the limbal palisades of Vogt. If the stem cells are destroyed due to chemical injury, healthy corneal epithelium will not fill the surface defects. This causes persistent epithelial defect and also invite vascularisation and ‘conjunctivalisation’ or growth of cells of conjunctival phenotype on the corneal surface. If there is a total or near total stem cell deficiency, the stem cells need to be transplanted to the affected eye. These stem cells are taken from another eye of the same patient.